
Professor Martin Bricknell, Dr Mohamed Gad, Dr Chiuyi Lin and Professor Christoph Meyer 1
The COVID pandemic has been the dominant issue for national governments and international organisations over the past year. Whilst originating as a threat to health, it has had implications across most ministries (health, economics, education, internal affairs, diplomacy, defence etc) and has affected many aspects of international relations including trade, supply chains, development assistance and conflict. Governments have mobilised all sources of national power, including their armed forces, as part of their crisis response. At the beginning of the crisis the comparative analogy between war and pandemics was widely cited. Most countries have used their armed forces to augment the civilian response, including their military medical services. Armed forces may provide a unique resource to governments as source of disciplined personnel under an established leadership system who can be directed to undertake new roles and tasks, in contrast to civilians who may not have the same terms of employment.
The contribution of armed forces has been underpinned by pre-existing civil-military relations, including the relative size and capacity of the military compared to other services controlled by national governments. Whilst there are unique aspects to the organisation of each country’s response, there are many potential areas of similarity and difference between countries that might inform lessons for health security policy and civil-military relations in the future. Within our programme of research into the health aspects of the security sector, civil-military relations and military medicine, we have sought to codify the contribution of security health services to wider national health economies. This includes the development of a common framework to describe military health systems in order to enable international comparisons.
Based on these foundations, we develop a structured approach to the comparative analysis of the civil-military aspects of the response to the COVID crisis between countries. Our research is based on the identification, collation and categorisation of reliable data to use as evidence. This Defence In-Depth report reviews the methods and conclusions of a series of studies that we have undertaken in this field and proposes a unifying typology of military medical activities that have been used by different countries to support their civilian health system to meet the needs of their populations affected by COVID. This typology will be useful as a foundation for further analysis of the civil-military response in order to identify those activities that might need to be sustained as part of preparedness for future pandemics, even if defence budgets might shrink as a result of the economic impact on government funding. Our publications are listed at the end of this report.
Methods
There are recognised qualitative and quantitative research methods for retrospectively describing and analysing organisational processes and outcomes such as documentary analysis, literature reviews, interviews, and statistical analysis of data. These will be useful for any inquiries and retrospective research.
However, it is more difficult to apply these research methods during the evolution of a crisis as the data is evolving and the individuals suitable for key informant interviews may not be available. Therefore, alternative primary sources are required. The identification, collation, analysis and interpretation should be as scientifically robust and rigorous as other methods. Our research programme aims to contribute to the knowledge of civil-military co-operation during the COVID crisis by systematically analysing press releases and other public documents from a selection of countries and international organisations (NATO, EU and UN) as part of a series of nested case studies. These case studies have provided a framework for our international comparisons of civil-military medical co-operation in the response to the COVID crisis. This work has evolved through a series of iterations as part of a research programme sequentially funded by King’s College London, NATO and the European Parliament.
The first phase of our research, conducted in Spring/Summer 2020, was an analysis of reports of the military contribution to the COVID response from 6 European countries (UK, France, Spain, Italy, Belgium and Sweden). This study developed our methodology for a structured and reproducible GoogleTM search for relevant open-source electronic grey literature files. We identified 19 distinct descriptive categories of civil–military cooperation extending across seven analytical themes. These findings were published in the BMJ Military Health journal.
The second phase, conducted in Summer/Autumn 2020, extended this case studies to include countries with large armed forces (USA, Russia, China and Brazil), and enhanced the method by reviewing all press releases from the Ministries of Defence for all of the countries covered by our research. This phase was funded by the NATO Open Perspectives Exchange Network and published by NATO Allied Command Transformation. The final analysis, within a project conducted on behalf of the European Parliament, refreshed the data to the end of 2020. This included some targeted Key Informant Interviews and interpreted the COVID response in the wider context of future European security and defence policy.
This report builds on these research projects by proposing a typology for civil-military medical co-operation that can be used as a framework to analyse the activities in any particular country. This not only identifies common activities as an indication of ‘best practice’ but also identifies gaps between countries that might indicate pre-existing limitations or areas for further development. We have cited examples of each activity within our typology as endnotes with a hyperlink to the press release published by the relevant country.
TYPOLOGY FOR CIVIL-MILITARY MEDICAL CO-OPERATION
Conceptual approach
Our work has identified a list of military activities that countries have undertaken in response to the COVID crisis. These can be divided into 3 groups: (1) actions to protect and care for military personnel at home and deployed abroad; (2) general military activities in support of non-health components of the COVID response (e.g. use of military aircraft for repatriation of citizens from overseas, use of military personnel for security duties to release police to implement COVID control measures); (3) military and military medical activities to support civilian health systems.
The typology described below covers the last of these groups, from three perspectives – community care, enabling activities and hospital care. It does not cover civil-military co-operation on international security missions. Our conceptual model is based on the military medical approach to summarising the evacuation of casualties, the Operational Patient Care pathway. This considers the whole system as a seamless, integrated and incremental pathway of care from point of injury through to return to duty. This model provides a structured approach to describing each step of clinical care of a COVID patient and listing examples of military contributions to this pathway.
Community Care
Figure 1 illustrates the flow of care for a patient in the community setting from societal protection measures through all steps until bio-psycho-social recovery, including potential admission to hospital if their condition requires it. Armed forces have contributed to civilian capacity across this pathway. At the level of protection, some countries have used armed forces personnel to reinforce civilian police in the imposition of restrictions of movement (lockdowns), quarantine and running ‘COVID hotels’. Military personnel have also provided augmentation to community testing including laboratory services and contact tracing.
More recently, military personnel have assisted vaccination programmes as these have rolled out. Whilst most of this assistance has been done by general duties military personnel, military medical personnel have provided specific augmentation to civilian ambulance services and primary care services, including the distribution of pharmaceuticals and essential care packages to COVID patients self-caring at home and isolated communities. The potential range of military medical support to hospital services is extensive and covered in Figure 2. Military medical services have also provided augmentation and training to out-of-hospital nursing and social care homes. Mortuary services are the final component of the system, and military personnel have augmented this sector in some countries.
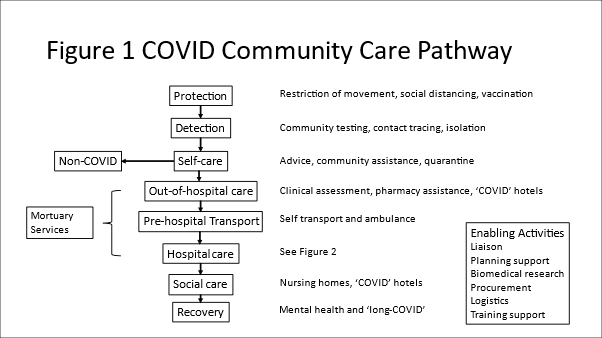
Enabling Activities
As shown in Figure 1, in addition to direct augmentation of clinical services, armed forces personnel have provided wider enabling activities in support of civilian health services. At the most basic level, this has included embedding military liaison officers within the civilian health management system to improve civil-military coordination. At a deeper level, military personnel have provided support to planning and the leadership of specific task groups, including supporting the regulation and movement of patients between hospitals using military assets. Some nations have a military biomedical research capacity that has contributed to different aspects of research in COVID, alongside using military personnel as an experimental population. Military medical personnel have also contributed to national and international training capacity in the use of personal protective equipment and clinical management of COVID patients.
Hospital Care
Hospitals are complex systems of systems. The same ‘care pathway’ approach is used to illustrate the potential roles of military medical services to augment the civilian hospital system and shown at Figure 2. Some nations have allowed civilians to access military hospitals, deployed military field hospitals, or converted existing buildings to augment local hospital networks. Staying at this level, military medical services have also provided ambulances, aeromedical aircraft and patient escort teams on trains and ships to assist in the movement of COVID patients between hospitals. At a tactical level, military medical personnel and teams have reinforced many components of a hospital’s clinical and support services to provide additional capacity and resilience within existing civilian hospitals. The mechanism for this reinforcement by military medical personnel has varied from provision of individuals to augment civilian teams (every case study), through to formed military teams taking over shifts or departments, to military personnel taking over the leadership of civilian hospitals.

DISCUSSION
The graphics at Figure 1 and 2 provide a typology that show the findings of our research into the types of military medical activities that have augmented civilian health systems. These summarise the accrued evidence that we found for at least one of these activities by one of the countries that we have studied, and indeed many of these activities were undertaken by most nations (e.g. use of military medical personnel to augment civilian hospitals and opening military hospitals to civilian COVID patients). No nation did every activity. This might be because we failed to detect a report of an activity, or the nation did not consider it, or explicitly decided not to do it. One example was providing access to military hospitals, which was not reported by the UK or Finland as these countries do not have military hospitals.
Countries with large military medical services deployed military field hospitals (e.g. Russia, France) or hospital ships (USA) to augment civilian health services. However, there is emerging evidence that providing additional personnel to existing facilities might be a better way to add capacity to the system as most hospital buildings have the space and equipment to expand services. It is noticeable that there are very few examples of temporary intensive care hospitals being used as anticipated at the time that they were established, though temporary facilities have had utility in providing ‘step-up COVID hotels’ or ‘step-down’ or low-level nursing care for COVID patients prior to their discharge from medical care in some countries (e.g. Spain). This illustrates the inter-relationship between health and social care, which has become even more important when considering the prevention of transmission of COVID between healthcare settings.
As illustrated by the example of military hospitals, it is likely that other wider factors influenced civil-military medical co-operation when comparing between countries. These may include pre-existing models for civil-military co-operation in times of crisis, the size and scale of the military health system relative its responsibilities for its beneficiaries and the wider civilian system, the pre-existing organisation and capacity of the civilian health system, and softer aspects of civil-military relationships and political power, including the relationships between national/federal, regional and local authorities. It will be important to identify and validate such factors in order to inform strategic choices for investment into mitigating the risk of future health crises affecting national and global security.
Finally, the process of research that informs the post-COVID inquiries and lessons learned should be underpinned by sufficient rigour that the data used represents a valid and reliable sample of the evidence. The nature of the evidence is likely to evolve as different forms of data become available. Our work shows how a structured approach to collating and analysing press reports can have contemporaneous value and provide an insight to developing the typologies and frameworks that can inform the search for other sources of evidence of activities that occurred during a crisis.
Acknowledgements
The authors would like to thank the other contributors to the research cited in this report including: Dr Sophia Besch, Dr Ramon Pacheco Pardo, Dr Zenobia Homan, Dr Adrian Gheorghe, Mr Joseph Kazibwe and Ms Emily Quirk.
This work was partially funded by: NATO Open Perspectives Exchange Network PO 204000836 and European Parliament Subcommittee on Security and Defence EP/EXPO/SEDE/FWC/2019–01/Lot4/1/C/07.
Bibliography
Bricknell M, Homan Z, Gheorghe A, Quirk E, Gad MM, Kazibwe J. Civil–military cooperation in the early response to the COVID-19 pandemic in six European countries. BMJ Military Health. 2021 Mar 31. https://doi.org/10.1136/bmjmilitary-2020-001721.
Bricknell M, Gad MM, Homan Z, Gheorghe A, Quirk E, Kazibwe J. An Analysis Of The National Responses To The COVID-19 Pandemic Through The Lens Of Medical Military Support Requirements. 5 ed. Norfolk, Virginia: NATO Allied Command Transformation, 2021. 100 p.
Meyer C, Bricknell M, Pacheco Pardo R. How the COVID-19 crisis has affected security and defence-related aspects of the EU: Part II – In Depth Analysis. 2021. 46 p. https://doi.org/10.2861/93636
Meyer C, Bricknell M, Besch S. How the COVID-19 crisis has affected security and defence-related aspects for the EU: Part I – Briefing. 2020. 19 p. https://doi.org/10.2861/906815 .
__________________________________
1 Professor Martin Bricknell is Professor of Conflict, Health and Military Medicine at the School of Security Studies, King’s College London; Dr Mohamed Gad is an Adviser to the Health Economics, Global Health and Development (GHD) group, School of Public Health, Imperial College London; Dr Chiuyi Lin is a Research Associate in the School of Security Studies, King’s College London; and Professor Christoph Meyer is Professor of European and International Politics, School of Politics and Economics, King’s College London.
